Drawbacks of Optical Internal Urethrotomy (OIU): Optical Internal Urethrotomy (OIU) has emerged as a popular minimally invasive treatment option for urethral strictures, offering patients relief from urinary symptoms associated with urethral narrowing. While OIU boasts advantages such as reduced invasiveness and shorter recovery times compared to traditional open surgical techniques, it is imperative to explore the potential disadvantages and limitations associated with this procedure. In this comprehensive exploration, we delve into the nuanced drawbacks of OIU, providing insights into its challenges and implications in urological practice.
Understanding Optical Internal Urethrotomy (OIU):
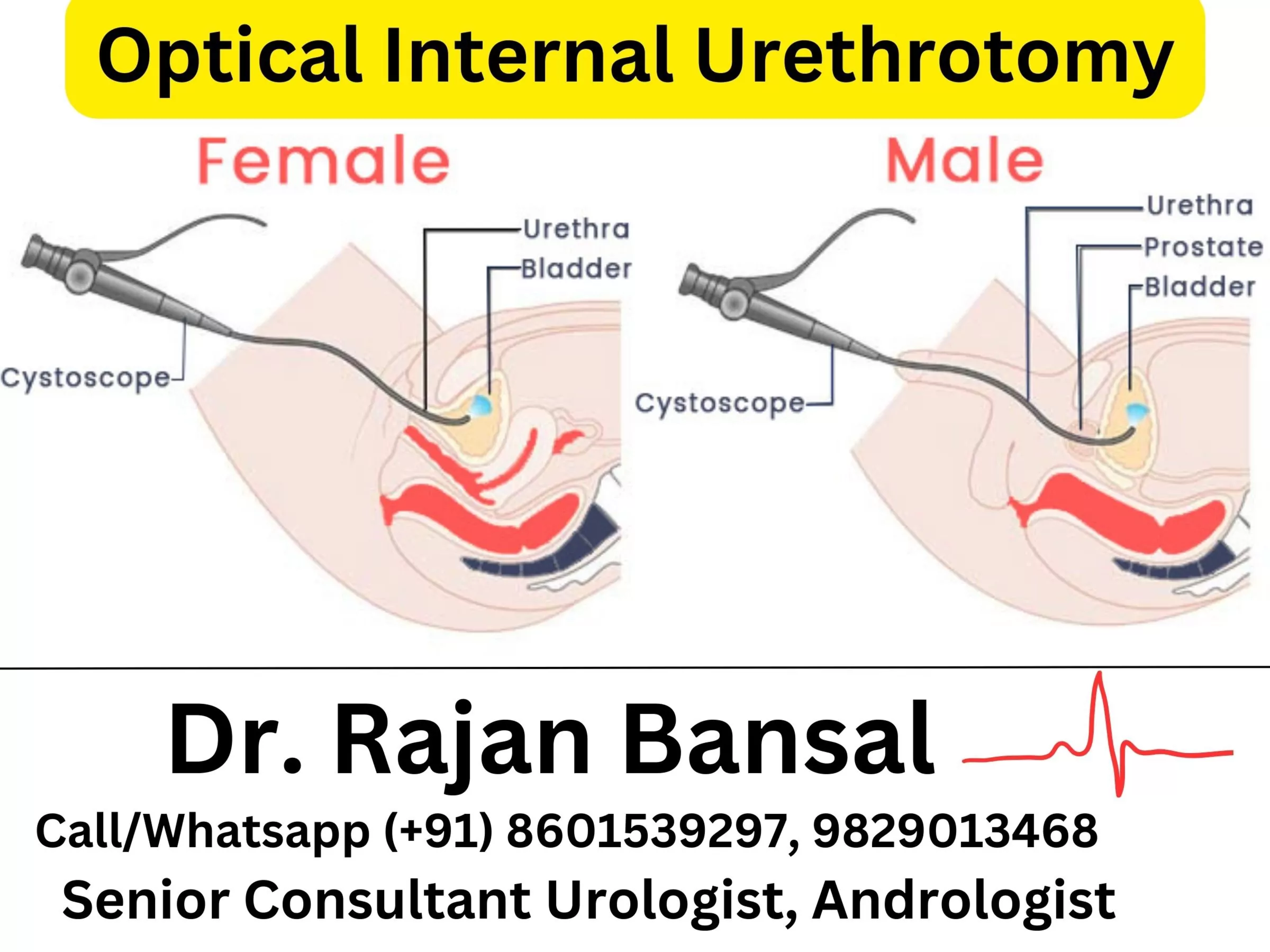
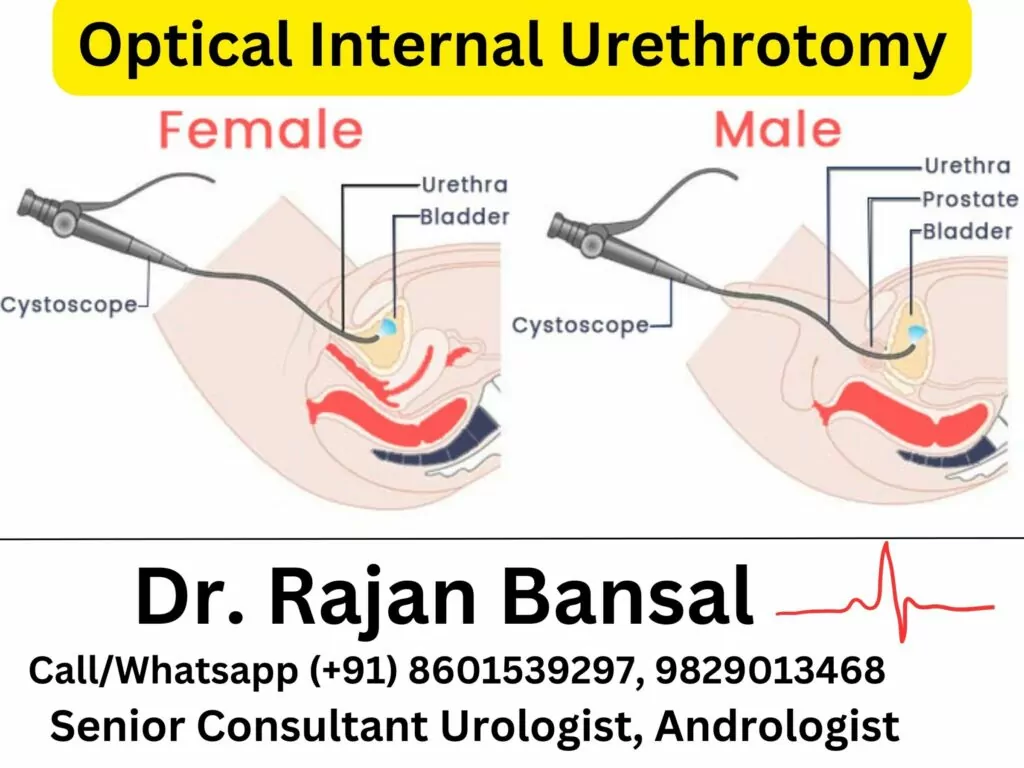
OIU involves the use of a specialized endoscope equipped with a light source and camera (urethrotome) to visualize and incise scar tissue within the urethra, thereby widening the narrowed segment and restoring urine flow. This outpatient procedure is typically performed under spinal or general anesthesia and offers the advantage of minimal tissue trauma and expedited recovery. While OIU is effective in addressing certain urethral strictures, its efficacy and safety profile warrant closer examination in light of potential drawbacks.
Disadvantages of Optical Internal Urethrotomy (OIU):
Stricture Recurrence:
A primary concern associated with OIU is the propensity for stricture recurrence following the procedure. Despite initial success in incising scar tissue and widening the urethral lumen, the natural healing process may lead to the reformation of scar tissue over time, resulting in recurrent narrowing of the urethra. Studies have reported recurrence rates ranging from 30% to 50% within the first year following OIU, necessitating repeat procedures or alternative treatment modalities [1, 2].
Risk of Complications:
OIU carries inherent risks of procedural complications, including bleeding, infection, urinary tract injury, and urethral perforation. While these complications are relatively rare, they can occur, particularly in cases of complex or recurrent strictures, or when the procedure is performed by less experienced surgeons. Vigilant monitoring and adherence to meticulous surgical technique are essential for mitigating the risk of adverse events associated with OIU [3].
Limited Efficacy in Complex Strictures:
Despite its efficacy in addressing certain urethral strictures, OIU may be less effective in treating complex cases characterized by extensive scar tissue or previous failed treatments. In such instances, the scar tissue may be too dense or extensive to adequately address with endoscopic incisions alone, necessitating more extensive surgical interventions such as urethroplasty. Additionally, OIU may yield suboptimal results in patients with inflammatory or radiation-induced strictures, where tissue healing is impaired [4].
Persistence of Urinary Symptoms:
While OIU aims to alleviate urinary symptoms associated with urethral strictures, some patients may continue to experience bothersome urinary symptoms despite successful dilation of the narrowed segment. This may be attributable to underlying bladder dysfunction or associated conditions such as overactive bladder or bladder outlet obstruction. In such cases, adjunctive management strategies may be required to address these residual symptoms and optimize patient outcomes [5].
Recurrent calibration procedures:
Another significant drawback of Optical Internal Urethrotomy (OIU) is the necessity for recurrent calibration procedures due to stricture recurrence over time. Despite the initial success of OIU in widening the urethral segment and alleviating urinary symptoms, studies have shown that scar tissue formation often leads to the re-narrowing of the urethra, necessitating periodic follow-up interventions or urethral dilation to maintain urethral patency and symptom relief [1, 2]. This requirement for repeated calibration procedures can impose a substantial burden on patients, potentially impacting their quality of life and leading to increased healthcare utilization. Moreover, each subsequent procedure carries inherent risks of complications, such as bleeding, infection, or urethral injury, highlighting the limitations of OIU in providing durable and definitive treatment for urethral strictures.
Conclusion:
While Optical Internal Urethrotomy (OIU) offers advantages in terms of minimal invasiveness and expedited recovery, it is essential to recognize its limitations and potential drawbacks. Stricture recurrence, procedural complications, limited efficacy in complex cases, and persistence of urinary symptoms are among the disadvantages associated with OIU. By understanding these nuances and considering patient-specific factors, urologists can make informed decisions regarding the optimal management approach for urethral strictures. Continued research efforts aimed at refining surgical techniques, optimizing patient selection criteria, and exploring novel treatment modalities are essential for further improving outcomes and mitigating the disadvantages associated with OIU.
Best Hospital for Stricture Urethra and Stricture Ureter Treatment – Institute of Urology, Jaipur, Rajasthan, India
For over 35 years, the Institute of Urology Hospital has been at the forefront of urological care, catering to the diverse needs of patients across all age groups and genders. With an unwavering commitment to excellence and a team of dedicated urologists, surgeons, and medical professionals, our hospital has become synonymous with high-quality care and patient satisfaction. By prioritizing individualized treatment plans and embracing the latest advancements in urology, we have earned the trust of our patients and established ourselves as the go-to destination for all urological concerns and men’s health-related issues. Our enduring legacy of excellence is a testament to our relentless pursuit of superior patient outcomes and our steadfast dedication to delivering compassionate and comprehensive care.
We have also started the facility of online consultation so that you can discuss about your problems in detail with our experts from the comfort of your home. Please remember to keep ready all the investigations that you’ve had done so far so that it is helpful for the specialist to guide you precisely about the next course of action. At Institute of Urology, we strictly abide by the International protocols so that we keep up with the latest and best of what the advancements in the medical field has to offer.
Our doctors can be reached Monday to Saturday during working hours.
Dr. M. Roychowdhury – 9929513468/ 9829013468
Dr. Rajan Bansal – 8601539297
References:
- Santucci RA, Mario LA, McAninch JW. Anastomotic urethroplasty for bulbar urethral stricture: analysis of 168 patients. J Urol. 2002; 167(4):1715-9.
- Barbagli G, Palminteri E, Guazzoni G, et al. Bulbar urethroplasty using buccal mucosa grafts placed on the ventral, dorsal or lateral surface of the urethra: are results affected by the surgical technique? J Urol. 2005; 174(3):955-7.
- Andrich DE, Mundy AR. What is the best technique for urethroplasty? Eur Urol. 2008; 54(5):1031-41.
- Erickson BA, Breyer BN, McAninch JW. Management of urethral strictures. Ther Adv Urol. 2012; 4(6):335-46.
- Morey AF, McAninch JW. When and how to use buccal mucosal grafts in adult bulbar urethroplasty. Urology. 1996; 48(2):194-8.