PCNL is a technique used to remove certain stones in the kidney or upper ureter (the tube that drains urine from the kidney to the bladder) that are too large for other forms of stone treatment such as shock wave lithotripsy or ureteroscopy.
What are the benefits of this procedure ?
With PCNL, large stones can be removed in a single operation in most cases and most patients recover and return to normal activity quickly.
Procedure:
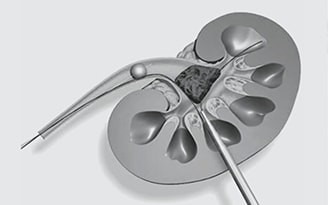
After general anaesthesia is given, a fine tube is placed inside the kidney through urinary passage. This tube is used to fill the kidney with a special dye seen on X – ray. This provides a clear “road map” picture to do the kidney puncture. The patient is then placed on his/ her abdomen and the kidney is located with X –ray. A needle puncture is made into the kidney and a wire inserted through this. The wire is used as guide to allow a tract to be dilated to about 1 cm across. A cut of 1.5 cm is needed on the skin for this. Once inside the kidney a telescope (nephroscope) is inserted and the stone is visualized. The stone is broken up into fragments as required and the fragments are removed. A tube is left in the kidney to allow easy drainage of urine.
As this is an invasive surgery kidney track heals with a tiny scar of a millimeter or so across. In the long term these are very insignificant changes and doesn’t have any effect on normal function of the kidney.
What are the possible complications?
Specific complications and their frequency are listed below. This does not include every possible complication but covers the more common or serious. Complications may also arise from anaeshesia and should be discussed with the anaesthetist. Generally speaking the risk of PCNL increase with the size of the stone, as operating times increase. Breaking up a large stone into removable fragments also increases the chance of some damage occurring to the kidney.
1) Bleeding – Some bleeding is normal but heavy bleeding is uncommon (1%).
- A) Early bleeding – If very severe a conversion to open sugary may be needed to stop the bleeding if all other measures fail. This is extremely rare.
- B) Later bleeding – (0.5 – 2%) This occurs if a communication develops between an artery and vein near the puncture site. It is treated with occlusion of the connection via a catheter through the groin. (selective renal angiography).
2) Infection: Infection of the urine is not uncommon before the operation. Some stones have bacteria trapped inside them which are released during the operation. Antibiotics are given routinely. This reduces the risk of infection. Severe infection occurs in around 0.25% patients.
3) Rare complication
- A) Bowel injury – an abnormality positioned bowel can be damaged during needle puncture. About 2% of people have this anomaly, but bowel injury is much less common.
- B) Lung Injury – Some time the needle puncture may traverse the lung. But extremely rare.
- C) Absorption of large fluid volumes May happen after a long procedure.
How successful is it ?
PCNL is the most effective means of treating large stones or stones in the lower pole of the kidney. A successful PCNL removes all the stones. The success of the operation is related to the stone size and stone position, ranging from 95% for lower pole stone to 90% for Staghorn stones. Other techniques may be preferable for different stone types and position. Choices include ESWL and Ureteroscopic laser stone ablation (RIRS).
How long does it take?
60 – 90 minutes. The does not include the time for the anaesthetist to put the patient to sleep or for the patient to wake up.
How long will the patient be in hospital?
Hospital stay is generally 2 – 3 days.
Are there any alternatives to surgery?
This should be discussed prior to operation. About 5% of stones are dissolvable without surgery. Not all stones need to be removed.
Is there any thing a patient needs to do before and after the operation?
Before surgery –
- Stop smoking. Several days of being smoke free reduces the risks of pneumonia and clots in the legs.
- Get some gentle exercise: fitter the patient faster will be the recovery.
- Eat lots of fruit and vegetables: to improve resistance to infections and to heal faster. Also prevents constipation.
After Surgery
- Drink plenty of fluids – this will make it easier and more comfortable to pass urine.
- Avoid constipation – straining to open bowels will increase the risk of bleeding
- Get out of bed – lying in bed causes pneumonia and clots in legs.
Are there any things a patient shouldn’t do?
- No heavy lifting/ straining for four weeks
- No driving until one can comfortably do everything on one’s own around the house.